I can’t access my account or I can’t reset my password.
Please email us at info@spinningbabies.com with your order number, using the same email you used to sign-up for your account.
I purchased a video and did not get my login credentials.
Thank you for your purchase. We are very sorry you have not been able to view your video. You should have received an email titled “Access your video!” with instructions and login credentials. Please search All Mail for this email as it sometimes is filtered to promotions or spam folders. If you are unable to locate your information please contact info@spinningbabies.com.
What’s the difference between the Parent Class video and the Daily Essentials video? Which one should I get?
With Daily Essentials, you will get a guided exercise routine that you can follow along with. With Parent Class, you will review some stretches you can do during pregnancy and labor and explanations about the physiology of birth, but it does not contain prenatal yoga instruction. If you still have questions, feel free to send us an email at info@spinningbabies.com.
I have purchased Daily Essentials and/or Parent Class, but clicking on the videos in the community portal takes me to the shop. How can I access my videos again?
One solution is to clear your browser’s cache. Here is a link to instructions on how to clear your cache in most common browsers: https://kb.iu.edu/d/ahic. Alternatively, you can use another browser to access the community site. If neither of these work, please email us at info@spinningbabies.com, and we’ll help you restore access to the videos.
Can I purchase Spinning Babies® digital products as a gift for someone else?
It is possible to buy a digital product for another recipient. Enter your information for billing but include the recipient’s email address for the delivery of the product. Please note: the email that contains the digital product may go to the recipient’s junk mail and therefore, they may not see it if they are not expecting anything from Spinning Babies®, so it’s nice to let them know that it is on its way.
What do I do if I purchased a video before August 2018 and I can’t access it?
If you have purchased a video before August 2018, the transaction would have been through Vimeo. Please reach out to us at info@spinningbabies.com.
Can I have a refund?
If there is an issue with a physical order, please reach out to us at info@spinningbabies.com. We do not offer refunds on digital products, including online courses.
What is Spinning Babies®?
Spinning Babies® is an approach based on easing baby’s rotation. When rotation is easier for baby, birth is often easier for mother.
The pelvis has three levels and each level may differ in where there is more space for baby’s head. Babies change position in labor to fit the pelvis. To make position changes easier for baby, we include muscle lengthening (toning not strengthening), body balancing, and increasing the measurements of each diameter of the pelvis, when helping labor be easier is a goal. Spinning Babies® develops a new paradigm for birth care for parents and for providers that is not cervix-centered or force-powered.
Is Spinning Babies® another way of saying Optimal Fetal Positioning?
Actually, no. Spinning Babies® is indebted to Midwife Jean Sutton, developer of Optimal Fetal Positioning.
Is Spinning Babies® invasive?
A midwife asked me if trying to influence the baby’s position wasn’t an intervention that is disturbing to the mother. Introducing mothers to the risks of posterior labor and the label of having a posterior fetus felt wrong to her. She said, “Let’s see what nature does.”
Now we know that 60% of first-time babies that are OP to start labor will change position before the end of labor. Several studies show that about 30% of the babies that were OP at the start of labor are OP at the end of labor.
Recent studies report about 8% of babies are OP at the time of delivery and not quite half of these are being born vaginally. The May 2005 Lieberman study showed 12% of babies from epidural births were OP at the end of labor compared to 3.3% of babies who were not exposed to epidurals. The OP labor may be long or short and, when born vaginally, the midwife can feel satisfied in her hands off approach–and so will I. However, the mother has one of the 30% of OP labors that need special help to finish she will move up the intervention ladder to Pitocin augmentation of labor (IV with medication to strengthen contractions), a vacuum or forceps delivery or major surgery. It is these mothers and babies that Spinning Babies® is designed for.
How do I become an affiliate?
If you would like to share links to the Spinning Babies® website and products on your own website or social media, you could earn an affiliate commission. Please fill out the affiliate request form. We will review your request and respond to you within 5 business days. All commissions earned through affiliate links will be paid via PayPal. You will need a PayPal account to receive your payout.
How do I get a Spinning Babies® workshop in my city?
Thank you for your interest to bringing Spinning Babies® to your community! Please review the requirements for hosting a workshop. If you are interested to host please click the form at the bottom of the web page and provide your information. We will review your request and, if possible, put you in touch with a Spinning Babies® Approved Trainer who can discuss with you how to organize a workshop.
What is the best position for baby to be in by the time labor begins?
The ideal, or optimal, fetal position is a flexed baby. We often hear that an optimal position is head down with baby’s back to your front or left. That’s because these are the most common positions associated with good spine flexion. A good fetal position aims the baby’s crown onto the cervix to help it open more easily and labor progress smoothly.
When babies start labor with the back of the head towards mother’s anterior (front) less rotation has to happen. A baby facing forward (posterior) or head up (breech) may present a challenge, or not. Spinning Babies® trains providers to discern why and when we need to intervene or when its fine to wait and trust.
A “malpositioned” baby is one that can’t enter the pelvis; lying sideways (transverse lie) or diagonally (oblique lie), or one that doesn’t fit as well because the chin is up.
Spinning Babies® helps baby get into position for birth and helps support a normal, even natural, childbirth.
My doctor/midwife suggested lying on my left side with my leg on a pillow (or ball) – is this Spinning Babies®?
Sleeping on the left side is good for blood circulation to the baby. Of course, mothers roll over, but spending more time on your left side than on your right, and very little time on your back is best. Studies show sleeping and resting on your left is a good thing for womb-babies.
But will lying on the left turn a posterior baby to anterior? Unlikely. Will it be good to do anyway? Yes.
Natural birth enthusiasts know the benefits of gravity (in this case, lying on the left) and movement on labor progress. But these aren’t enough when modern lifestyle issues limit the baby’s flexion and position. Spinning Babies® promotes certain exercises and professionals to help bring the pelvis back into balance. Everyone can use a little more balance. But some of us need a little more.
After a set of balancing activities, such as the four myofascial techniques in the website here, and other activities, resting on the left with a pillow between both the knees and the ankles, is a lovely way to rest. Leaning over slightly with the leg supported to prevent a twist in the hip muscles is better.
I’ve had (or heard of) a posterior baby going well, so what’s the fuss?
There’s more to labor ease than which way the baby faces in the pelvis.
Both breech and posterior fetal positions can be born by natural birth. Spontaneous birth is more likely when baby’s chin is tucked. A woman can more readily navigate a long labor when family and providers know how to support rotation and wellbeing.
Some posterior labors have the challenge of fetal extension, the baby’s back is straight and the full top of the head is entering the pelvis instead of the more mold-able crown. About half of all posterior babies are born vaginally. Which half might you be in? You can move towards the easier end of the spectrum with body balancing, and even professional body work in pregnancy and labor. Using Spinning Babies® Labor Progress tips throughout the labor section of this website and on the Spinning Babies® Parent Class will help you avoid an unnecessary surgery for your baby’s birth.
Can Spinning Babies®’ suggestions put a baby who is in a good position into a bad position?
The benefits of all the usual Spinning Babies® techniques are good for anterior starting positions as well as the posterior starting positions. The usual techniques will not typically put an anterior baby who is in a good position already into a poor position. Hundreds, if not thousands, of women are doing inversions now, as you read this, and not having their head down babies go breech. Many are reporting more comfort and easier births.
There have been 4-5 cases in the years of this website (since 2002 and this is 2016 when I am writing this sentence) that I have gotten feedback that the forward-leaning inversion caused a head down baby to back up and go either breech or transverse. The women who told me about it chose to continue the suggested exercises and in 2-5 days their babies were again head down.
I think this is because a tight ligament is loosened but not balanced and temporarily makes the lower uterine segment unstable and so the baby comes up. By finishing the balance restoration that was begun the baby now finds room to settle head down again and this time without the chronic tension or torsion. Some of these women had a history of hard labors before and two were first time mothers.
Read the contraindications carefully and the instructions carefully, don’t simply try to imitate the photo or you will miss important safety considerations.
Are there techniques or positions that we shouldn’t use?
Some of the special circumstances techniques should not be used unless the fetal position is known!
Proceed under your own advice. Women have been inverting with yoga for decades. While I know of no study for statistics ongoing upside down in pregnancy with a head-down baby and having the baby flip breech, it may happen rarely. On the other hand, 3-5% (yes, 5%) of American babies are breech at term, so one in 20 is potentially breech and that means they flip breech at some point, not always in the second trimester, but the third trimester, too.
The question has to be, do babies flip breech less often or more often if mother’s do a 30-second inversion once a day throughout pregnancy.
I know that these moms doing daily inversions are reporting less discomfort and lots of breeches, though not all, are flipping head down.
Is there any harm in going upside down?
I am inclined to say no, not when the Forward-Leaning Inversion is done with these directions. But you should know first:
If you say yes to any of these, then NO inversions. These would be reasons not to get upside down without someone involved who is highly skilled in fetal monitoring, such as an experienced Labor and Delivery nurse.
There are many ways of doing any technique. “Overdoing it” is not appropriate. A few techniques are only used in pregnancy for a breech baby and not a head-down baby. The Open Knee-chest for more than a couple minutes or not at all for a woman with the above contraindications, for example.
Don’t get the mistaken idea that if a little time inverted is good, than a long time is better. The Forward-Leaning Inversion is meant to be done for a very short time, the time to get a stretch in the uterosacral ligament, so I suggest only 30 seconds. A baby who is not engaged, the woman who has several pregnancies before, the woman with extra fluid– may end up breech if the inversion is held a long time without contractions to keep baby head down.
The activities listed for “all” women are typically safe, when done as described, meaning these activities are recommended for all healthy women who do not have pregnancy or birthing risks. Check with an experienced midwife or doctor; or a physical therapist who specializes in helping pregnant women.
When might your suggested activities not work?
Habits of poor posture and chronic tension affect the balance (symmetry, abdominal tone and the state of tension or relaxation) over time. The uterus works most effectively when the abdominal ligaments, muscles and fascia (a strong coating of membrane around all the organs, are in balance.
Active women who walk, swim or did regular yoga may have overcome many of the bad effects of growing up sitting in school desks or slouching on the couch.
When we have had a habit for years, sitting and standing properly for a few weeks is not likely to correct the effects. A history of intense dance, sports, or core strengthening, or a car accident or other twist and stop event can make restoring balance challenging.
That’s where body balancing with myofascial techniques come in. Spinning Babies® teaches some of Dr. Carol Phillips’ techniques to parents and professionals and Rebozo sifting, a traditional Mexican technique with the long scarf. Together these are called the
Fantastic Four and they can be used in pregnancy and even in labor appropriately.
Professional help may make all the difference. Find the person right for you to get body work from.
Your technique isn’t working – is it the baby’s fault or the mother’s fault?
This is a trick question. It’s just not helpful to think of fetal position as being anyone’s fault. In a long labor, a mother may ask “Why doesn’t this baby come out?” A helper might joke, “This is a stubborn baby.” Midwives have been heard to say, “This mother is too much in her head” or “She’s too uptight.” Actually, there are two rebozo jiggling activities on this website that soften the muscles and take the mother into a more heightened parasympathetic state (out of her head).
A mother does her best given the baby’s position and the time and support available. So, while emotional or mental tension can certainly lengthen a birth, midwives and doctors seldom realize how much a slight malposition of the baby plays in labor progress.
Mothers are often blamed for birth complications, when the lack of support in a birth-phobic society has left her neglected, lacking in the knowledge she desires to have and from access to wise care. The mother, too, is doing her best in the situation she lives in.
After a long labor ended in a cesarean, a mother asks, “Am I broken?” Sometimes it’s a matter of the baby’s head being the wrong way in. The pelvis would have birthed the baby with the chin tucked and crown first, but perhaps couldn’t fit a baby whose chin was up or head was tilted.
Baby is trying to accommodate the space available the womb. Muscle tension or laxity pulls on the lower uterus making less room. The womb may not aim into the pelvis smoothly. A baby will take the most optimal position possible.
Some providers know how to help reposition baby and some do not. The same solution doesn’t work for every variation, so the cause and effect can seem random. When understanding anatomy of the soft tissues with angle of the head and pelvic shape, the light comes on and a pattern emerges.
“But, Gail, my friend’s doctor (could also be a midwife or nurse) didn’t let her get out of bed, and she had a cesarean for a long labor. Isn’t that the doctor’s fault?
It isn’t the doctor’s wish to have a mother suffer. Doctors also practice in a dynamic interaction of hospital administration, colleagues, and limits to training in natural birth solutions. Perspectives in what makes a cesarean necessary or acceptable may differ.
A woman who feels that she had a cesarean for a less than absolute necessity sometimes comes to feel mislead by her sense of trust in routine medical care. Assumptions are exposed painfully. Anger is an appropriate emotion when we are forced to change our plans beyond our expectations, especially without our voice in the decision. We all do the best we can given the variables of the day.
We can prevent the blame and shame spiral if we take time to find three things:
A mother may be told her baby is in a good position for birth only to find out later that head down is not enough. Learning about fetal position is something the mother, herself, must pursue. Relying on medical and midwifery helpers, even bodyworkers, may not serve every mother’s needs.
As humans we are, well, human. Everyone is doing the best they can with the knowledge, emotional safety, and time they have within the culture they live and move in.
Which babies need the extra help to get into position?
Which babies are those that need this extra help? How can we know if we are “watering the rain” or really doing something that helps the baby? As a midwife in a small practice, I am able to feel each woman’s baby through her abdomen at each prenatal throughout her prenatal check ups. Somewhere around 26 to 31 weeks I can usually tell the position of a baby’s head and tell which way the baby is facing.
By this continuity of care, I notice which babies are held tightly into position by tight uterine ligaments or by low amniotic fluid levels (a less common reason). If the baby doesn’t shift around for comfort and stretching, if the baby feels locked in place and if this baby is on the right or directly posterior, the chances of a difficult birth are higher. Even if we can’t get the baby to swing around to rest the back of their head in the mother’s left side, we can start to loosen up the ligaments and pelvic joints, help the chin to tuck and encourage the flexibility needed for labor contractions to do their part in fetal rotation. See The Long Labor That Wasn’t in the Birth Stories section of this website.
These situations are more likely to be among first-time moms, older first-time moms or women experiencing their first labors after previous cesareans without advanced labor in their past experience.
When the baby is OP and the water breaks before contractions, she is at higher risk for surgery. If she has her water broke by a provider before the baby engages, rotates or descends she is also at higher risk for cesarean.
If the OP baby is not engaged (dropped) before labor begins she is at higher risk. Especially if she doesn’t use the specific activities, many listed in Spinning Babies®, to address the issues of her particular birth.
When should one start Spinning Babies® activities?
Starting good posture before pregnancy is best, really in childhood. While we’re on the topic of children, can we stop the habit of putting developing bodies into restrictive chairs for long hours and for over 12 years of school? We’ve grown up with our backs restricted all day, then ride home in bucket style seating, only to slouch in front of the television or more sitting in front of a computer. Plus, a lack of sunlight (Vitamin D) is causing increasing rates of pelvis-twisting rickets.
In pregnancy, practice good posture as soon as you learn of the benefits.
A study based on ultrasound images through pregnancy show that fetal positioning begins after the 10th week of pregnancy! Most babies have chosen their final birthing position at the end of the second trimester. My observations show that by 31 weeks most first-time babies are in position. The small number of breech babies becomes a smaller number until 3-4% are still breech at term (40 weeks). For some babies, whether breech or posterior, it will take more than good posture to change. Second babies may be able to use the mother’s gravity friendly positions to change until about 34-37 weeks. A few babies are exceptions to this and can change their position even in labor.
Most women begin their search for birth knowledge in the last trimester. Many times there will be enough time for the determined mother. When the pelvic brim is not round and the baby is posterior it might be too late to get the baby in a good starting position by maternal positioning alone. Other things can be done in the last weeks of pregnancy.
Will baby flip head up?
Sometimes women wonder if baby will flip head up, or breech, from doing an inversion.
I haven’t heard of this happening to a head-down baby when the pregnant woman does a short forward-leaning inversion. There is no reason to do a longer inversion if baby is not breech. Repeating inversions more often is better than doing them for a long time.
Some women who do yoga will like to do yoga inversions for longer than 30 seconds. I don’t know of a study showing whether “yoginis” (women who do yoga regularly) have a higher or lower rate of breech. I believe, but don’t have the data, that pelvic and myofascial symmetry (muscle and fascia) reduces breech presentation. You decide what is best for you and consult a midwife or doctor to help you decide if you aren’t sure. A hands-on abdominal exam will help determine whether your abdomen is extra soft, roomy, or your uterus is holding enough extra water to let baby flip more easily than average. On average, babies don’t flip easily.
You can ask your midwives and/or doctors if you have an unstable lie, high blood pressure, or polyhydramnios or any reason they can think of not to do a Forward-Leaning Inversion.
If your baby was breech (head up) and is now head down you can stop the inversions for a few days and walk briskly for a mile or more a day for three days. Continue to do balancing activities and anything specific to your situation.
How does Spinning Babies® make birth easier?
Babies settle in the easiest position they can before, and during birth. In labor, they begin from that position to turn to rotate through the pelvis… like a key unlocking the door. Easier rotation may mean an easier labor.
Since most babies can be born naturally, shouldn’t we wait to see? True, many women will have a normal birth with a passive approach. But unfortunately, more women today find themselves unexpectedly on the surgical table after labor did not progress. True, women are designed for birth, but modern life presents challenges. A large minority of birthing women (15-30% perhaps) may experience some type of intervention because of their baby’s position.
Spinning Babies® leads women through activities in pregnancy to prepare for a straightforward, even easier birth. Muscles that may have gotten short and tight from sitting and driving or a previous accident are lengthened and softened. In labor, there are techniques to help this and to open the pelvis right where baby needs some extra space. Labor progress is more than waiting for the cervix to open.
Mother’s job is to dilate; Baby’s job is to rotate!
The spectrum of ease in giving birth ranges from the dream birth to the greatest challenge. Most women will find that labor is good, rewarding work. Satisfaction increases with knowledgeable support by loving, listening, and skilled birth attendants, including midwives. More than 24 controlled studies show far more natural birth, fewer cesareans, and improved birth satisfaction with the continuous presence of a doula. (Repeat that last sentence to yourselves.)
Do you trust birth? Can I trust my body for my upcoming birth?
I do believe we can trust birth. I believe we can enjoy labor. I did, and I believe you can, too. I also believe that the way we prepare for natural birth with today’s lifestyles means we have to address the physical results of today’s lifestyles (shorter hamstrings, more pelvic instability (pain in SI and symphysis joints) and larger mothers and babies.
My previous birth was hard, what about this one?
Many women have a much easier birth the second time. The first baby seems to have left road signs telling the future babies where to turn.
The exceptions are few, and these are usually when a significant soft tissue injury occurred in the woman’s past, even in childhood, but perhaps between pregnancies.
Another situation which can make a subsequent birth hard would be a large baby and a truly small pelvis. Add a posterior or asynclitic (tipped head) baby and there may be a long labor.
Balance the body when either of these situations occur and you will see a great improvement in the birth process.
Combine Active Birth principles with a really good pregnancy diet (healthy food choices, not low calorie) and you can improve chances of a straightforward labor even more.
Check out the Lamaze 6 birth practices for a better birth experience while you are working towards a better birth experience.
Whether you had a cesarean, vacuum or spontaneous birth, whether you had a breech or posterior baby before, you can bring about a better balance, better nutrition and lifestyle habits, and better support for a birth to look forward to. Please don’t be afraid. You have much to look forward to! Labor is worth it!
What if I do the exercises and try for a natural labor and it doesn’t work, and I have a cesarean? Won’t I be disappointed?
If you find you need an intervention, cesarean, vacuum extraction, or medications, I hope you feel you did all you could -without suffering- for a birth closest to nature possible.
This website seeks to reassure all birthing women, and the professionals and paraprofessionals (doulas, childbirth educators) who help them, regardless of how they “do birth.” That said, you will see my bias and my bias is birth!
What’s the matter with a cesarean?
Sometimes we accept there is a time to intervene in a particular birth. Cesareans are a life saver; but should not be a lifestyle. Major surgery has its own set of risks, including injury and even death. Most cesareans are safe today, but involve anesthesia, incisions, blood loss, and too often, infection. Many births are now managed with cesarean surgery even before labor begins!
Some labors do need to finish with a surgical birth, but most don’t. There are benefits to the birth process in the mind and hormones of mother and child. Please give labor a chance. A baby gets more preparation for breathing and living in air if labor was part of the journey, even when a cesarean was, too.
Together, we can reduce the tide of surgical birth and return birth to the mother’s own abilities.
Wondering if the search for physiologic birth is worth it? Project yourself to a year from now, will you be able to reflect that you did everything you could to be aware, to grow, and to become the mother you hoped to be? Take the time to learn. Fetal Positioning and body balancing are rather new concepts, so don’t expect a doula, nurse, or even your doctor or midwife to tell you “all you need to know.”
The most important thing is love.
How should I prepare for birth after a previous cesarean for lack of engagement?
Here are some recommendations for a pregnancy after a previous labor finished via cesarean due to lack of engagement (baby’s head had remained high and didn’t come into the pelvis):
The classical suggestion of long, steady, almost brisk, walks still has many benefits. For some women walking daily is not enough. But realize, to walk well, wear flat, comfortable shoes, swing from the thigh and hold your neck long with the crown of your head to the sky, shoulders back and, of course, no tucking the bum.
Visit Aligned and Well for pregnancy-focused tips on posture, walking, standing, and squatting. It’s a treasure trove! You will understand more after visiting Katy Bowman online.
Use smart Maternal Positioning. See Rest Smart on Spinning Babies.
Please look at the Chiropractor/Myofascial Release/Craniosacral Therapist and even Maya Massage explanations on this website under Professional Help.
Chiropractic techniques may also be done by some Osteopaths. In some areas of the world, you might find an Osteopath for the same purposes.
These helpers will help you obtain maximum pelvic stability and Balance.
If you have migraines, tight jaw or grinding teeth and other things affecting your neck and head, have a bodyworker and use self-care for those areas, too, to help your pelvis “open”. It may have been open, I can’t say, of course, but an open, balanced pelvic alignment is the goal.
Achieving full balance and flexibility, helps you eliminate a potential tightness or twist affecting the brim of your pelvis (and everything else). Continually refreshing your balance with daily activities and regular professional bodywork helps make the most open, balanced pelvis you can achieve. Do the Daily Do’s and Weekly Activities, too, according to safety for you (if you don’t have contraindications for some, such as high blood pressure or placental bleeding).
This way, you can eliminate the question of whether your babies didn’t engage because of something you could have done something about, or due to a pelvis that is actually “too small”, in your case, at the brim.
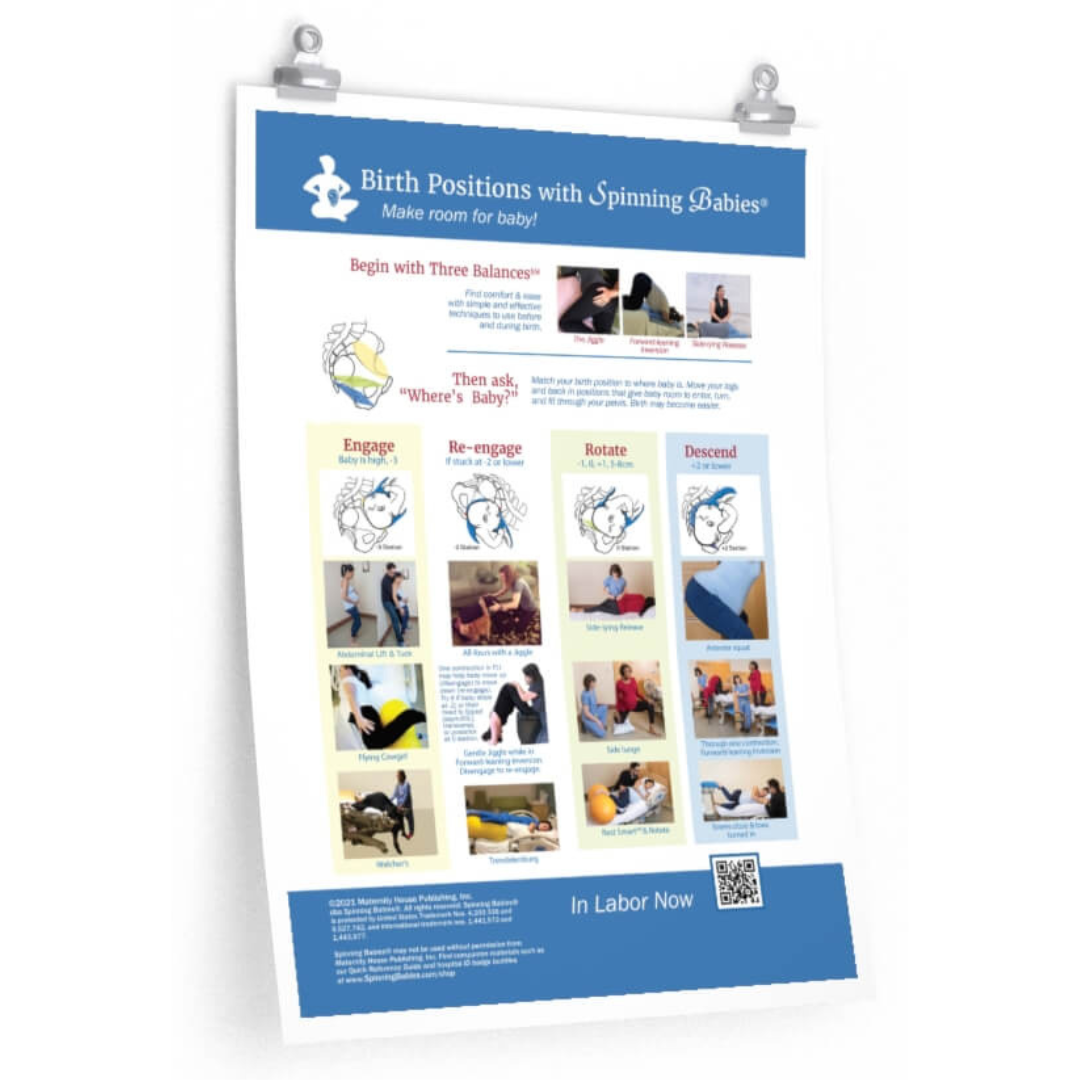
With contractions, using the Abdominal Lift and Tuck for ten contractions first, and if that doesn’t engage baby, then Walcher’s Open The Brim technique. Do those with your midwife/doctor present because it is possible that once baby engages, if labor is already active, that birth could be rather soon afterwards, although it usually just gets things back on track for whatever stage of labor you were in when you did them, early or late labor.
Moving freely in these ways and eating lots of fresh veggies, with lots of greens and drinking fresh, pure water (no bubbles and avoid toxic plastic bottles, please) are ways of improving your chances.
The benefits of laboring are worth the challenge of finding the providers and making the arrangements to be supported for laboring. Whether you labor and push your baby out or whether you labor and have another cesarean, labor helps prepare both baby and mama for brain and blood chemical changes for the next stages of their lives.
My hope is that you are supported and validated in your wise choices and you listen to your body and your baby without ideology, fear, or exclusion of choices. Only you can be present with what you need, now, and at the time of birth.
Should I get induced to reduce risks caused by a big baby?
There are several reasons to get induced for labor, but baby’s size is not one of them. An increase in cesarean birth is one risk, and oxygen deprivation is another. Estimating fetal size is not particularly accurate. The chance of having a slightly premature (called a late preterm) baby is much higher with induction. The March of Dimes warns that babies even a couple weeks early are twice as likely to die in the first year of life than babies that go to their due dates. Natural labor may protect babies that are a couple weeks early, but induced labor does not allow the fetus the same maturing hormones as natural labor. Several studies show that healthy babies are not more likely to die at 41 and 42 weeks as previously thought when looking only at one study that included some health problems. Induction does not protect against shoulder dystocia and may increase it. The common “reasons” for inducing a woman with a baby that is suspected to be large are not so reasonable after all. Find out if there is any medical reason not to go into labor on your own. Not because of statistics, but because of your own personal health status.
Mothers are concerned that the larger baby will hurt more to be born or cause more pelvic floor damage. Very large babies can be associated with higher rates of tearing as the head and shoulders come out, especially if you do have an episiotomy or give birth on your back. But tears and episiotomies (the vagina is cut open by the doctor or midwife) happen when birthing small babies, too. Patience and good skin tone allow many 11-pounders to birth without a tear. Lying on one’s back forces the head into the perineum, so don’t birth on your back. A first-time mom with a big baby may not want to be on her back, even semi-sitting, when the head comes out. Tears and cuts are more likely with obstetricians than family practice doctors or midwives.
Urinary incontinence is said to be higher among women that gave birth vaginally. And that may be true, but not by significantly greater numbers. Pushing before the urge, having a pudendal block, and use of a vacuum or forceps each increases pelvic floor damage. Nuns and men also have urinary incontinence. A little leaking is more common among all groups of people who are over 50. And the term urinary incontinence doesn’t mean you have to wear diapers to have the phrase applied to you. Just one sneeze and dribble gets you in the group of pants wetters.
Doctors are concerned that a large baby will have trouble birthing the shoulders. About 8 in 100 babies near 9 pounds can need help from the doctor or midwife for their shoulders to be born. When babies are over 10-pounds it may be one in ten babies experience shoulder dystocia (stuck). However, neither labor inductions nor preventative cesareans have been shown to reduce the number of cases of stuck shoulders.
After birth, studies show labor induction for fetal size doesn’t prevent complications and may add other troubles stemming from the intervention of induction. Inductions are more likely to end in cesareans than spontaneous birth.
My doctor told me my baby was posterior and large, should I just have a cesarean?
There are no studies that show that the risks of surgery are less than going into labor with a large baby when mother and baby are otherwise healthy. There are studies that show the risk of surgery is higher than vaginal birth for healthy mothers and babies.
Most posterior babies rotate in labor sometime before their head is born. It is more important whether, when you are a first-time birther, baby’s chin is tucked to their chest. Such a baby has a flexed head. Flexion allows rotation more easily than a chin-up baby. Body work, hula-hooping on the birth ball, walking and belly dancing all help the chin tuck. Work on this in the third trimester of pregnancy so baby’s head is flexed by 38 weeks.
Even if a woman labors and then needs a cesarean, her baby will be blessed with benefits of labor. The cesarean for a head-down baby in labor that is not fitting the pelvis is not usually an emergency cesarean because the baby is unlikely to have a sudden emergency in such a scenario when the mother is getting good care. Monitoring will help the doctor/midwife know if labor is hard on the baby. The best strategy for a long labor is addressing the tension or torsion in the muscles with our recommended body balancing techniques; good labor nutrition; rest without drugs when tired; freedom of movement; a sense of humor and lots of patience. Body Balancing with our Three Balances before or to complement strong labor using good movement and smarter birth positions can be tried before assuming the baby won’t fit. Pauses in labor are common while the head molds.
Which side should I sleep on?
Research now suggests that falling asleep and/or waking up on the left, both or either, is protective of baby’s wellbeing.
Meanwhile, balancing out what is too tight in pelvic muscles and ligaments will help baby move towards the left in several days or weeks of the daily exercises shown here, or may take professional help to accomplish in pregnancy. A well-working metabolism helps, and walking and movement with a whole-food, low-sugar (or no sugar) diet helps your metabolism.
I also highly recommend that when you lie on your side that you use a pillow between your knee AND your ankle. Don’t let your ankle “hang” without support as this twists the uterine ligaments.
Switch sides when it’s uncomfortable. Getting up to go to the bathroom is shown to be protective of baby’s well-being, so don’t get too frustrated with getting up at night.
If your doctor recommends you sleep on your left side because you have high blood pressure, that’s another matter. I’ll stay out of that discussion.
For fetal position, the balance is on the inside. Attend to that and which side you sleep on will be less important – and more comfortable.
Should I sit on a pillow while driving my car?
It’s better to do balancing exercises after getting out of your car than changing the angle of your seating. The Standing Sacral Release is an excellent antidote for long rides in the car.
If you lift your buttocks up on a pillow or towel in the car and then need to stop suddenly you will be thrown into the steering wheel. The bucket seat is a protective angle to reduce this during sudden stops at low speeds.
You can sit on a deflated therapy ball, the 9″ small size, when it is placed front to back (like a menstrual pad) and allow your sitz bones to remain on the seat of the car.
Is it dangerous to negotiate with a doctor? What if I make the wrong decision?
Statistics show that not all common medical recommendations are leading to better outcomes.
Sometimes doctors and midwives do what is convenient or locally acceptable, even if studies show it is not the best choice. After all, sometimes you make a decision on what is easier for your family or partner to accept rather than what seems best for you. We are all human. On the other hand, you are an individual and not a group. Your situation is individual. You will make decisions on the information you have and the support you feel in either staying with the medical routine or asking for individual care for what is best for you and your baby. Being a responsible adult means taking the risk of doing the wrong thing. You can change your mind, you can change it back. You can see how far you get.
Most of the time when we are under stress, they pick what their loved ones and the experts are comfortable with, not necessarily what makes sense logically or intuitively to them. Stress causes most of us to draw close to one another. If your support people rely on routines for their sense of safety it will be hard for you in labor to stay out of their comfort zone.
If I ask the doctor or midwife to do something different, will I lose their support when I need them the most?
Your doctor and midwife want you to have a positive birth memory. They want to help you to have a safe and healthy birth. You want that too. When you differ on how that will happen, most often it is because the medical staff doesn’t realize what things will help you have a happy memory.
Staff are busy with many, many tasks and can often forget what a monumental day this is for you. Just remind them and let them feel that they can be your hero. Humor works for some, and respectful talk works for everyone. A Birth Plan helps the medical staff understand how they can add personal touches to the sometimes routine care in a busy hospital.
Just because you asked for a change from the usual routine doesn’t mean the doctor or midwife will punish you or stop being respectful. Talk about it. If you are worried, state your worry. You can say, “Doctor, I want to continue to work with you but I do not want to be induced early (or whatever your concern is). What else can we do to meet your concerns and what are you willing to do to meet mine?”
Ask:
Make a relationship with your caregiver by being open and talking about your concerns, but also about what you would like to see happen. If you are flexible and willing to change if medical needs become apparent, then the caregivers will see you are willing to work with them. They know that they can help you with the skills they have.
If you want something different than the skills your doctor has, you may need to bring in a person who does. A doula can help you with the goal of a natural birth, for instance, when an obstetrician may be willing to support that goal, but not have the time or training to give practical help.
Sometimes, you may have to change caregivers to find someone who can work respectfully with you. When you look back at your birth in five years, do you want to remember a respectful relationship or being afraid to change? But talk to your doctor first, don’t assume they can’t support a change. It is up to you to bring it up and follow it up.
What can I do to have a healthy-sized baby?
Eat a good diet throughout pregnancy of leafy green veggies for the placenta, a gallon of water each 24 hours for your vital organs and the amniotic fluid levels, lean protein sources such as whole eggs, chicken, millet, tempeh, and beef to reach 4-6 servings a day. A serving is two eggs, a piece of meat the size of a deck of cards, 15 raw almonds, etc. Have salt to your taste. Don’t avoid salt in pregnancy.
Avoid the ice cream, white flours, white rice, and candy. Eat fruit and nuts and take a good walk almost every day, or dance for 20 minutes if you can’t leave the house or have toddlers. Don’t go hungry, but eat smart. A sugary diet does make a baby big from unhealthy foods. White flour or soft wheat bread is much like a sugar snack once it is in your body. Again, it’s the position of baby’s head that is more important than size.
Ask your doctor if your baby’s health can be monitored as you go into labor on your own. Each case is individual and no website can make medical decisions for you. You will have to talk to your doctor or midwife to discuss what is best. Speaking up is part of parenting your child.
My client or I had an adverse outcome after using Spinning Babies®.
Please use this form to report the details of your adverse reaction and someone will be in touch after reviewing. We collect this information for our quality and safety improvement efforts. Your insight plays a vital role in our ongoing efforts to improve.
For additional education to even further enhance your pregnancy and labor preparation, shop our extensive collection of digital downloads, videos, DVDs, workbooks, and more.